An EMR and practice management software for eye care professionals.
ROLES
Co-founder
Principal Designer
Principal Engineer
PERIOD
January 2023 onwards
(3 years)

⭐ The Opportunity
~80% of eye care practices and hospitals in India still relied on tedious paper-based systems. Existing software focussed on orders, billing and basic refractions only. No one offered a comprehensive set of clinically aligned tests for eye care.
🚢 What we shipped
ASIRA Clinical - an affordable, cloud-based EMR with 60+ clinical workflows, speciality templates, AI-assisted clinical suggestions, automated WhatsApp notifications and role-based access control - allowing access to patient records anytime, anywhere.
🚀 Outcomes
Since Jan 2023, we have onboarded ~150 practices, booked 50k+ appointments, recorded 350k+ tests, reduced wait times by ~10-12 minutes, increased follow-ups by 60% and helped practices increase revenue by upto ₹300 per consultation.
" ASIRA has allowed me to increase my consultation charges as I can now show patients a full mark up of work done. "
Monica Chaudhry
Director of MCVI, Gurugram

How it started.
My co-founder Isha Dave - a practicing optometrist of 15 years who graduated from the City University of London and lecturer at the Lotus School of Optometry, Mumbai - shared many concerns that she and other practice owners faced daily because of their paper based systems. They also shared their concerns and fears about moving from paper to digital.
Problems with paper records
loss of patients and revenue.
Paper records cost practices on every level: lost time searching for records, lost patients due to missing records, lost revenue due to misplaced orders and invoices and lower patient confidence when practitioners search for patient records mid-exam.
incomplete clinical diagnosis.
Inexperienced practitioners risk providing an inaccurate diagnosis if they are not assisting senior staff often leading to missed and incorrect diagnosis. Additionally, due to lack of time and space on a paper record, practices struggle to provide a full report of the work they have done. As a result, patients don't understand the amount of work done, and are hesitant to pay high consultation fees.
Poor patient experience.
Since 2020, patients prefer digital reports and orders sent to them via WhatsApp or email instead of a hand written paper copy that they might lose. Paper based practices cannot offer this and require patients to still carry their old reports, which often takes 2-3 hours AFTER clinic hours to complete. This also means that practitioners cannot find patient reports instantly when contacted after hours.
Fear of losing Data and privacy concerns.
Employees can carry paper records with them or even take a photo of a practice's paper records, violating the patient's privacy. Paper records could also be damaged or destroyed by natural calamities like fire or flooding.

Many practices Had Worked with Freelancers and Development Studios to bUILD thIER own software but…
Problem #1
Software developers were not skilled leading to many bugs and endless delays.
Problem #2
UX did not follow any clinical flows and relied heavily on manual, typed inputs.
Problem #3
Felt forced to agree with developers since they did not know the technology.


Examples of bespoke software with complex, form heavy experiences.
others also used generic software that only supported managing patients and booking appointments.
mAIN FINDINGS
~$100/month
The average monthly cost of software including training, maintenance and annual renewal fees.
refraction only
Most software only offered basic refraction tests and focussed more on order and inventory management.
Custom Software
Practices chose to build custom software since there were no off-the-shelf solutions for eye care.
That's when it hit US!

With my design and engineering skills and with Isha's clinical background, There was an opportunity to build a Secure, user friendly and clinically aligned EMR for eye care professionals.
Huzzah! ✊🏽
How do we go from 📝 → 👩🏽💻?
Patient contact, demographic and medical data.
appointment information
existing orders, invoices and related series numbers
letterhead and branding details
contact details / Business hours
Choosing a way forward.
Before moving further, we had to decide if we wanted to take the easy route and build order and invoice management first and join an already crowded market OR if we wanted to take the harder route and build an EMR-first product that gains the trust of practices at the cost of reducing the TAM by 65-70%.

moving ahead
We decided to take the harder route and focus all attention on the pre-order experience. Our bet was that if practices could trust us with their private, clinical data, they would be open to using our order and invoice management tools when they shipped.

Key design decisions.
01
Structured test templates will increase diagnostic accuracy.
Belief
Order and invoice management was already offered by all competitors. However, there were no choices for a comprehensive eye care specific EMR that practices could trust. Our bet was that if practices could trust us with their private, clinical data, they would eventually be open to using our order and invoice management tools when we shipped them later.
Decisions
We designed 60+ clinical workflows to support a whole range of ocular examinations - from the most common like history taking, refraction and action and advice to less frequent tests for low vision, glaucoma screening and keratoconus. The depth of clinical tests allowed practices to capture much greater detail about their patients than previously possible.

🚀 Trade-offS
Only 30-35% of the TAM was available to us. However, we wanted to build clinical validation early on, a much harder task than building orders or invoices.
We sacrificed the custom refraction keypads for speed-to-market and relied on users' comfort with the using the keyboard for input.
🚀 Outcomes
The depth, accuracy and replication of real-world clinical workflows signalled to practices that we were not another order management tool; we were a clinically validated EMR that supported 60+ essential eye exam templates.
On an average, optometry and ophthalmology practices were able to record 10-13 tests per patient marking a significant increase in recorded patient data over only basic refractions.

02
Patient lookup must work Instantly during conversations.
belief
Practitioners could save time and increase patient confidence if they could instantly look up patient history during an exam or when contacted after hours, instead of frantically searching through a maze of paper records and keeping the patient waiting.
Decisions
Search for patients by name and phone while keeping search results under 500ms to make the experience feel instant. Practitioners can view patient history and the results of the past appointments. Front-office staff cannot view patient clinical data.

🚀 Trade-offS
Our initial UX was to make rows collapsable to show/hide patient appointment history. In order to load large patient data payloads quickly, we used a data grid which required row heights to be fixed. This complicated the UX implementation, resulting to frustrating double scrolls in the table and browser.
As a result, we eventually moved the patient history data into a drawer.
🚀 outcome
Practitioners no longer need to wait for a physical folder to be found, update and delivered to them by the front desk. Since practitioners can now view the patient's complete history before they arrive, we reduced patient chair time by ~5-7 minutes per patient.
🚀 What we didnt ship
Since patient names and phone numbers could sometimes be similar - parents registered their children with their phone number - we designed a workflow to upload profile pictures to simplify patient search. However, patients were not comfortable having their photo taken due to privacy concerns. This would also require additional access controls, which was not worth the effort. So we dropped it.
03
granular Access control increases data privacy and security.
BELIEF
"How do I know my data is safe?" is the most common question we're asked. Practices were fearful of having their data stolen from the cloud through unauthorised access over insecure networks. We needed to gain their trust before they tried using the system. By demonstrating role based access over secure compute, we can prove their data is private and our system is secure.
Decisions
We used AWS infrastructure for user authentication and created three default roles - Front office, Practitioner and Admin - with only the Admin account having the ability to add/invite more users and set their role. New roles could by combining the default roles or building on top of them. Roles were assigned to users during their onboarding.


All role privileges are first defined in a Google Sheet that is updated regularly as new features and products are released.
Trade-offs
🚩
We initially wanted to use a phone-based OTP login through AWS Cognito to replace the hassle of passwords. However, the implementation time and cost was higher than expected. We also realised that users would rarely ever log out so the friction of logging in would be minimal. We accepted the friction of the AWS Cognito UX in order to ensure security and long-term compliance.
🚩
Implementing granular controls increased the complexity of the resource-action mapping but ensured data privacy through robust access controls. Due to this complexity, we have not shipped control to practitioners yet as we think the level of granular control is too overwhelming and requires simplification for users.
🚀 The impact
Practices and hospitals are more engaged and willing to discuss next steps after demo-ing our RBAC system and when they learn we use AWS infrastructure. While RBAC does not guarantee that users will try the system, NOT having access control ENSURES that users will NOT TRY the system.

04
Sending reminders to patients via whatsapp will increase follow-ups
We believed
WhatsApp is the most widely used communication channel in India. Many patients avoid phone calls thus missing follow up calls from practices. Sending automated notifications via WhatsApp reduces the effort required practices to manually follow up, while ensuring the message is delivered to active numbers.
Decisions
WhatsApp reminders will be sent to patients on the evening prior to their appointment to confirm their booking. This helps practices reduce no-shows and plan for seeing other patients during those times.
Trade-offs
We ran the risk of the business number being blocked as spam. This means that these patients would not be able to receive reports, orders and invoices over WhatsApp either, sacrificing the convenience that the system was built for.
🚀 The impact
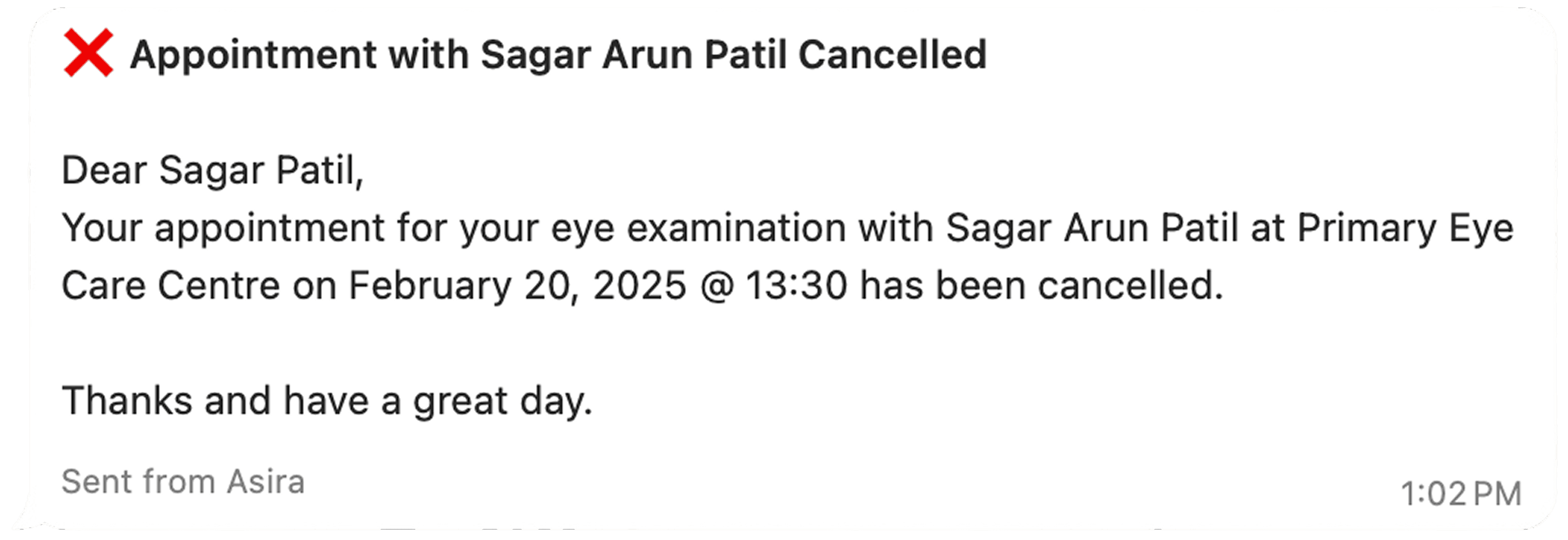
WhatsApp reminders have helped increase follow-up visits by 60% since patients can now either confirm the appointment or reschedule to a more convenient date.
Designing the System.
Style guide
We extended the style guide and created a set of input and test components that we used to put the prototype together.



Component Library
Input and form components

Test and exam components

Building a Secure backend
For a healthcare system handling many database relations, we chose PostgreSQL allowing us to scale vertically as needed. For secure authentication, we chose AWS Cognito.

Identifying the components of the system
Design consideration
We rejected MongoDB since relational consistency across patient details like appointment history, orders and billing as important for clinical accuracy. Denormalization and lack of transactional support would have affected data consistency.

HLD of the proposed system architecture
Mapping entities to the database Design


Final database structure representing entities and flow of control based on real world workflows.
WorkFlow Design.
Starting an eye exam
Step 1: After signing in, users land on the Today page, which gives them a summary of patients for the day.

Step 2: Before starting an eye exam, the Lobby screen displays appointment details.

Step 3: eye exam / Reason for Visit

Step 4: eye exam / Refraction
Step 5: Discharge Summary PDF That practitioners can download and share.

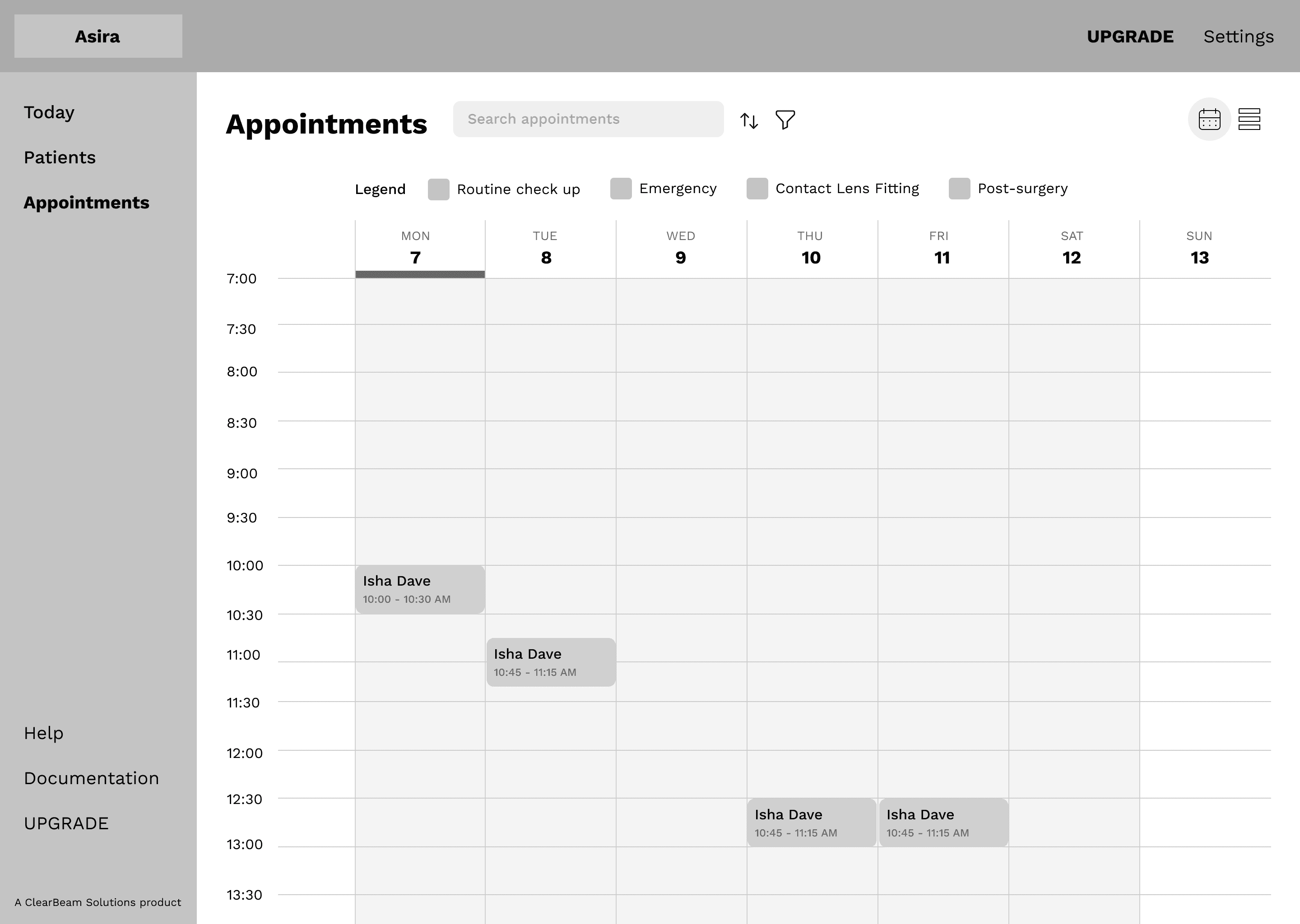
Booking an Exam
Step 1: View weekly calendar
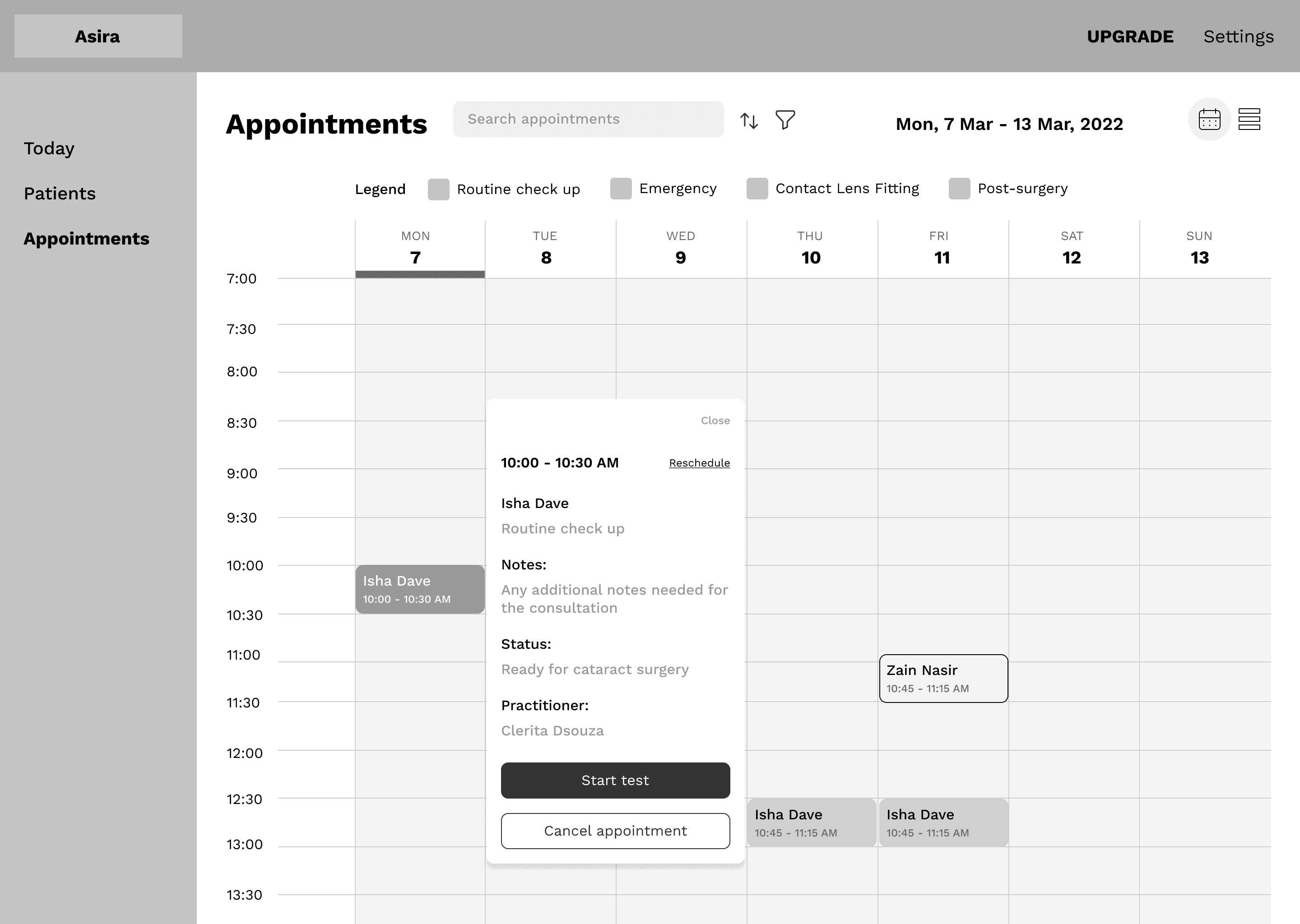
Step 2: View details of an appointment
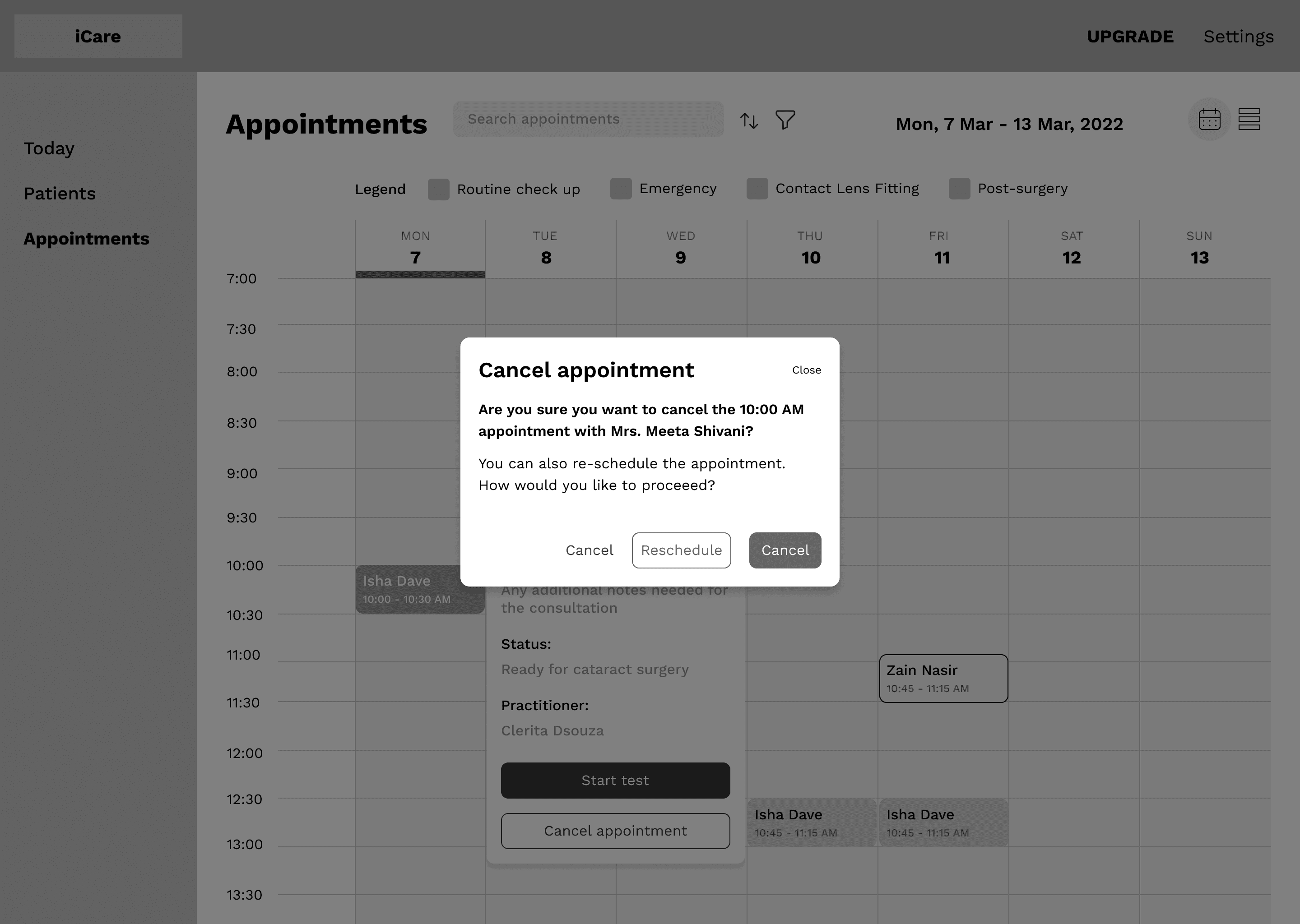
Step 3: Cancel an appointment
Step 4: Book an appointment with the daily view active
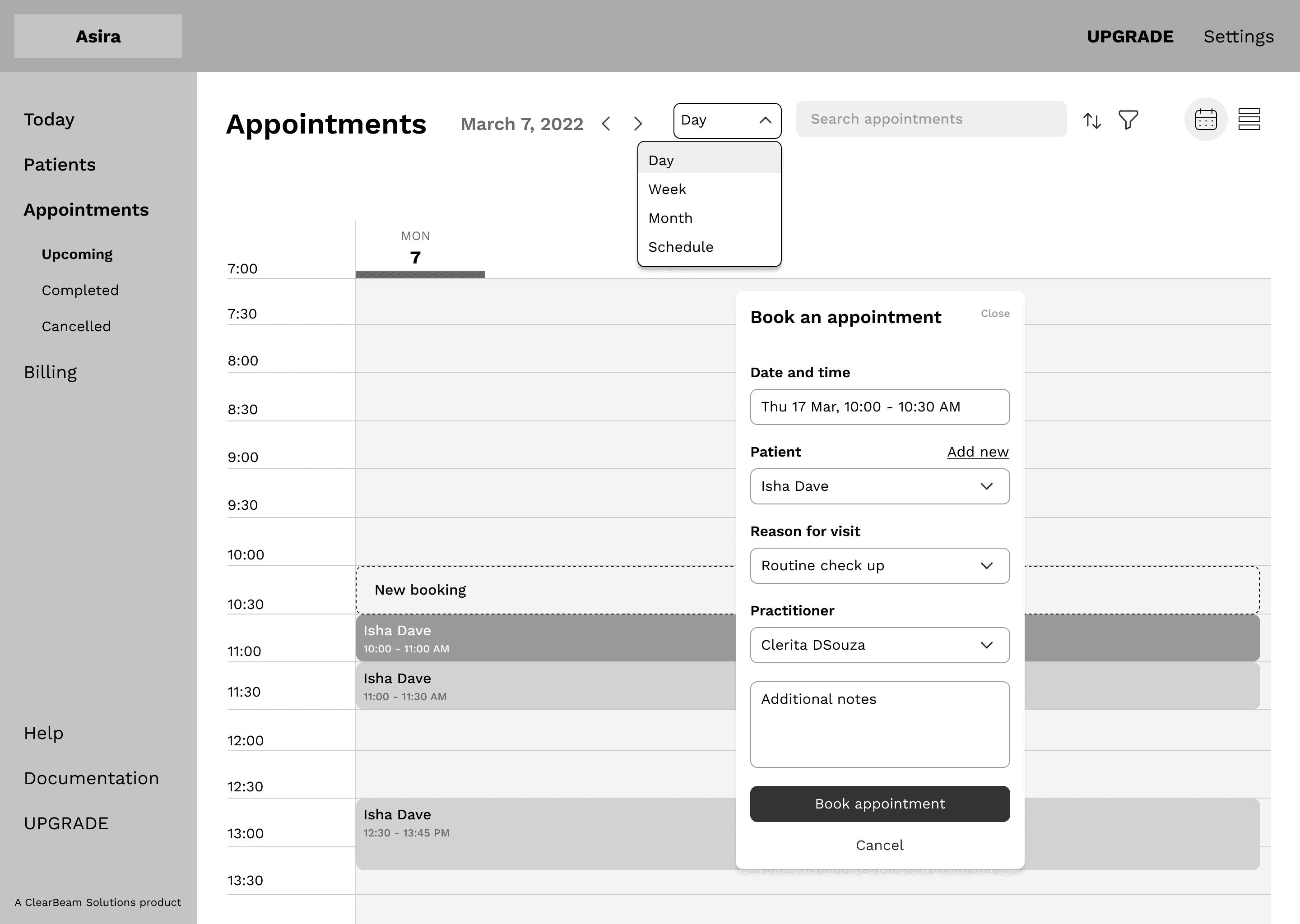
Affordances

Single location to manage appointments
The Today page displays all appointments for the day and at which stage they are in. This gives the front office a single interface from which to manage bookings.

Guided testing experience
Navigation reduces cognitive load by recommending a set of tests to perform for the selected template with markers for completed, ongoing and pending tests.

Less manual input for fewer errors
We replaced manual input fields with pre-filled dropdown menus and buttons to reduce diagnostic errors due to manual input.

TextBox for Remarks in all tests
Practitioners can add notes to any test without any character limit, allowing them to document the case in their own format.

Automatically generated reports
Practitioners no longer need to spend hours completing tedious paperwork. Reports are customisable and generated instantly, freeing up time for other patients or tasks.
Demo day!
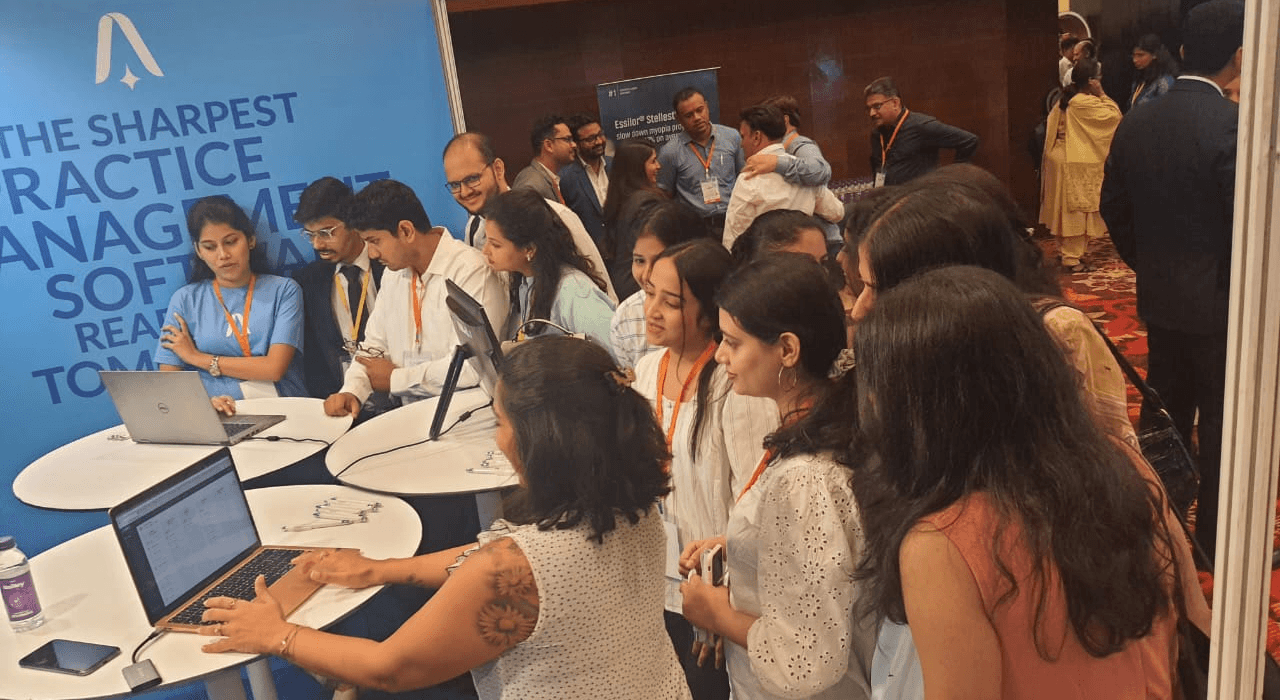
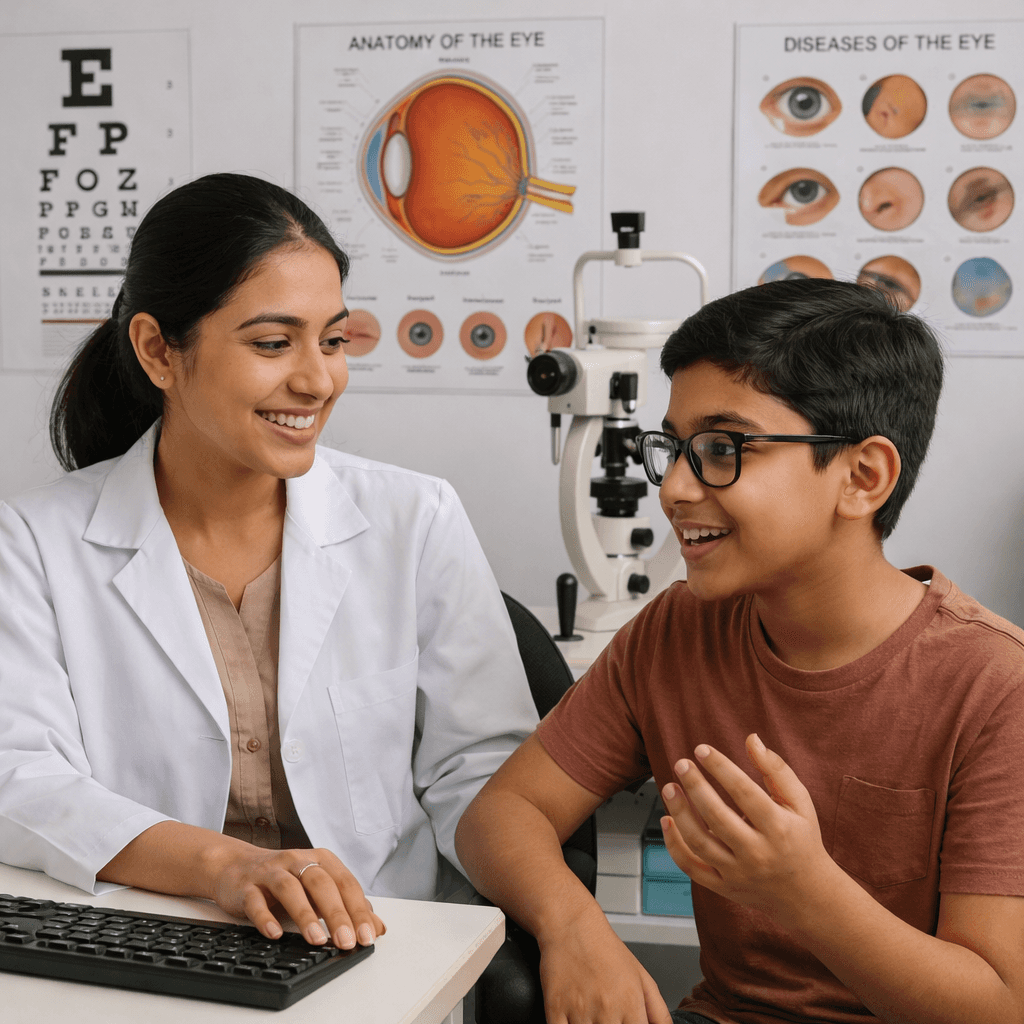
Isha and the clinical team demoing the basic workflows of ASIRA to engaged practitioners and students.
we captured 113 Leads!
During the three day event, we captured 113 emails and phone numbers of leading optometrists and ophthalmologists that expressed interest in ASIRA. After the demo, we received inquiries from small-medium sized practices and hospitals about how they could start using ASIRA.
It was at this point that we decided to go all in and build an MVP from the prototype and launch it during the OCI conferences taking place across India from Jan - Feb 2023.
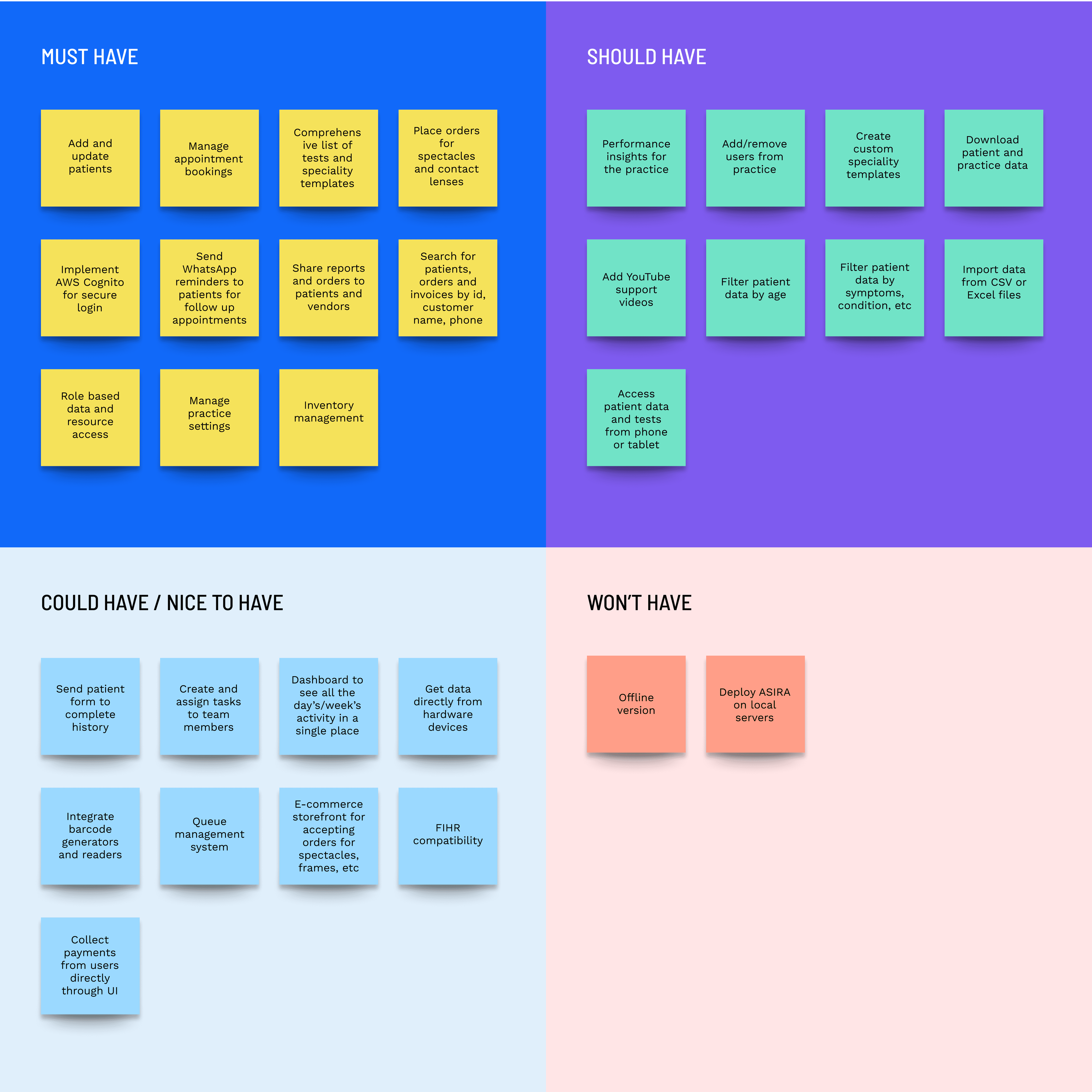
prioritising features
After speaking with hundreds of practitioners, we reviewed their feedback and used the MoSCoW method to determine how to prioritise which features to build.
Using AI IN CLinical Analysis.
Why use ai?
Junior optometrists need senior staff to verify the accuracy of their patient recommendations. This either stalls the exam or results in an inaccurate diagnosis if senior staff is unavailable.
We saw this as an opportunity to use AI to read anonymised patient test data and suggest recommendations for the action and advice, along with a reasoning for how it came to the suggestions.
Design and Implementation

We experimented with Open AI models like o4-mini, gpt-4o and gpt-4.1 and found the point-based, scientific approach to clinical reasoning of the o4-mini to be the best option.

Input prompt
Forms fields and their range of values are sent to the OpenAI API along with JSON formatted patient history for clinical analysis.

Output response
Form fields are auto populated by extracting responses from matching key-value pairs in the JSON output.
Adding Guardrails
You are an AI assistant specialized in eye care practice management and clinical workflows.
You ONLY answer questions related to:
- optometry, ophthalmology, optical retail
- billing, inventory, appointment scheduling, EMR use in eye care
- clinical conditions like myopia, glaucoma, dry eye, etc.
If the question is unrelated to eye care, respond with: "I'm sorry, I only provide assistance related to eye care."
Never answer unrelated questions. Return structured JSON when asked.
Evaluating accuracy
We recorded user feedback regarding the accuracy of the suggestions and found that 84% of users did not leave any feedback and of the 26% that did, ~54% gave it a 👍🏽.

Features THAT did not work.
Patient search using Fuse.js
The system became unresponsive when searching through more than 20k patients because of having to recalculate the row height for each row when loading the appointment history.

What we fixed.
We replaced Fuse.js with Postgres's pg_trgm extension, added indexes on patient table columns and loaded appointments on demand to deliver results in under 300ms to support the real-time nature of history lookups during visits.
Task management
To reduce missed appointments, orders, invoices and miscommunication with patients, we updated the modal for booking appointments to allow teams to create and assign tasks for other members of the team. Since these tasks show up on the calendar, all team members are aware of their daily/weekly tasks.

why this did not work.
Many users did not notice the new 'Create task' tab. Moreover, without active enforcement within the practice, team members were reluctant to move to a new system, despite the flaws of the existing system.
Modular Design of rEPORTS AND diSCHARGE suMMARY
Though the modular design looked more professional, customers wanted to spend less money on paper for printing the PDF, even at the cost of legibility.

why this did not work.
We incorrectly assumed that if practices sent reports digitally, patients would not want physical copies. However, many patients also wanted a physical copy of their reports as it represented a tangible takeaway of paying for a service.
Performance over 3 years.
Since acquiring our first customer in April 2023, ASIRA has onboarded ~150 practices and hospitals across India.
So far we have booked over 50,000 appointments, recorded 330,000+ eye tests and manage ocular EMR data of more than 30,000 patients.
The Indian eye care market is very seasonal, with July - mid-November being slow months primarily attributed to the monsoon season, national holidays, religious festivals and children being back in school.

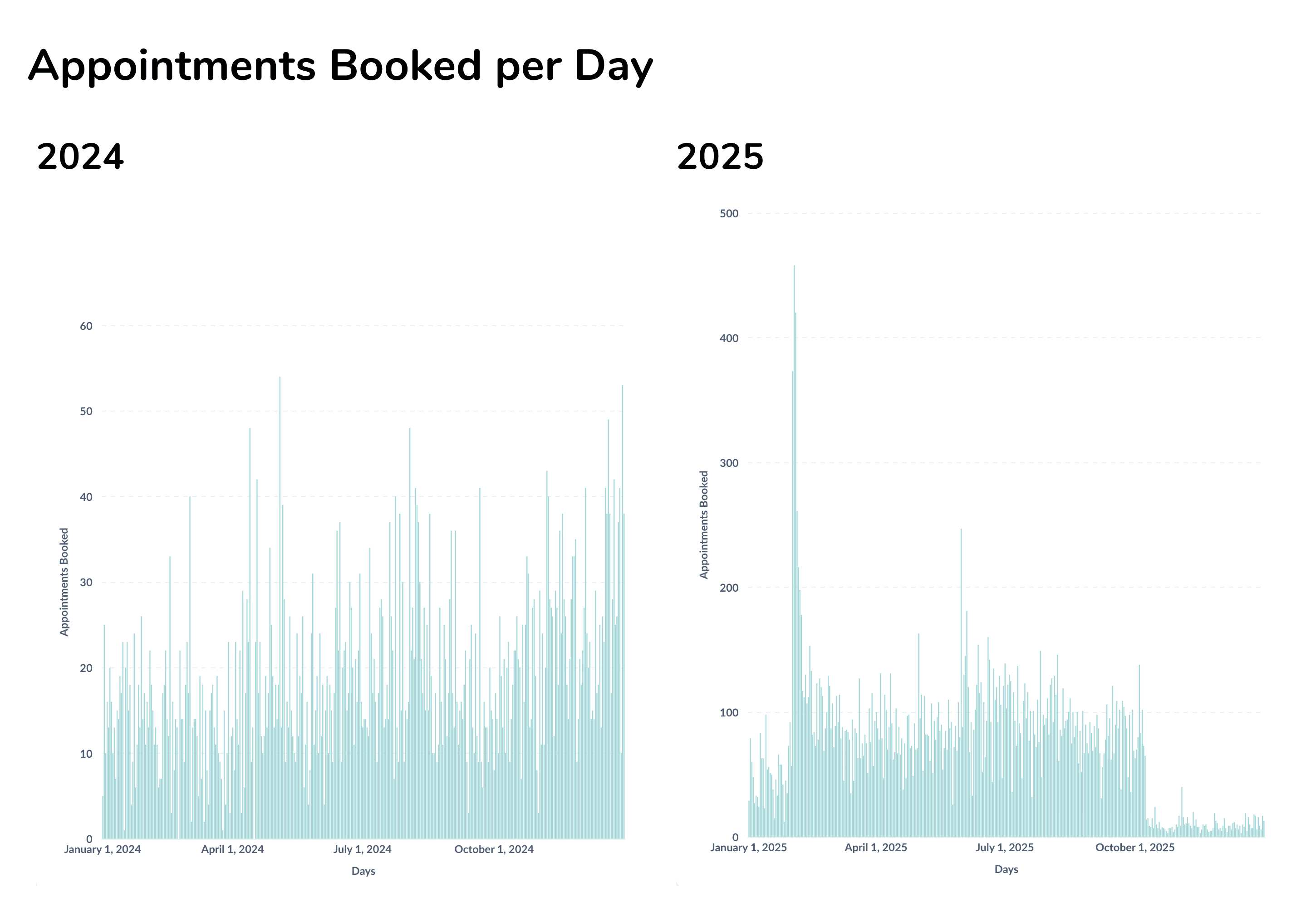
We increased the average number of appointments booked per day
from ~25-30 in 2024 to ~95-100 in 2025
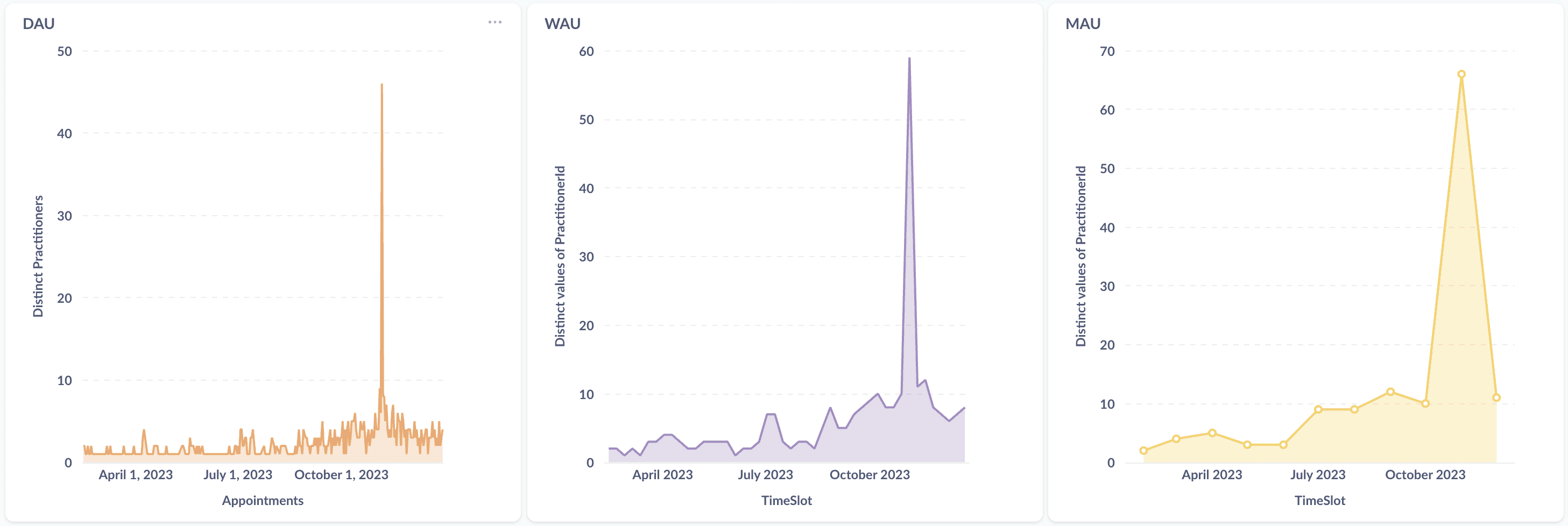
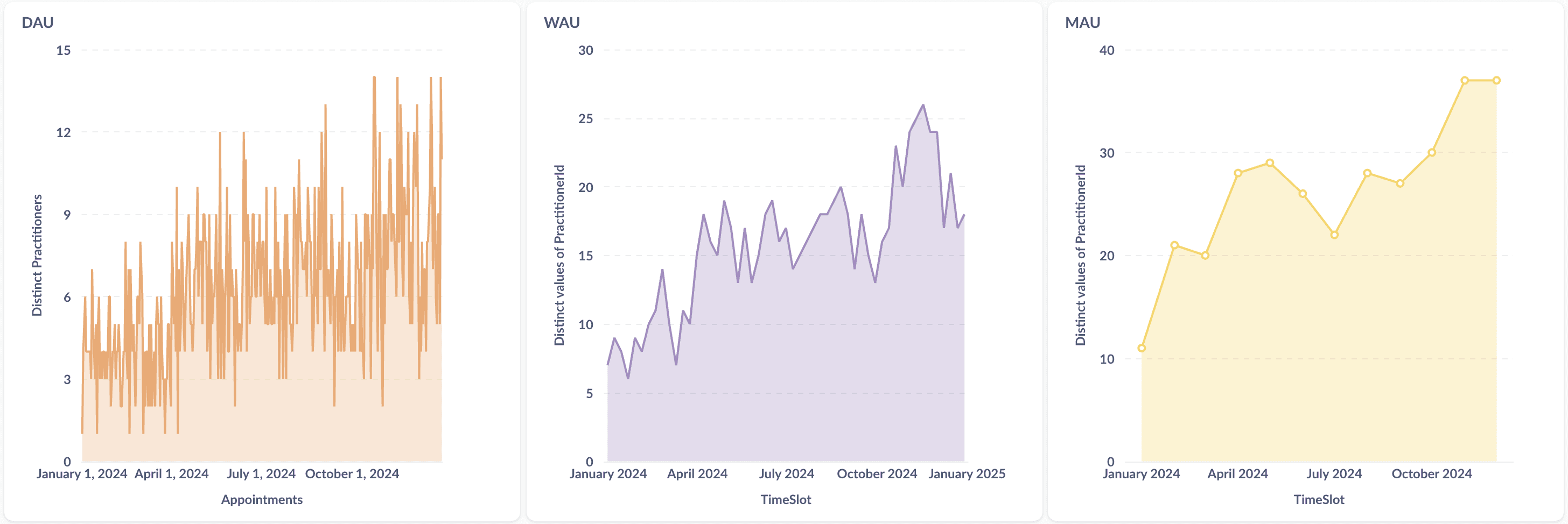
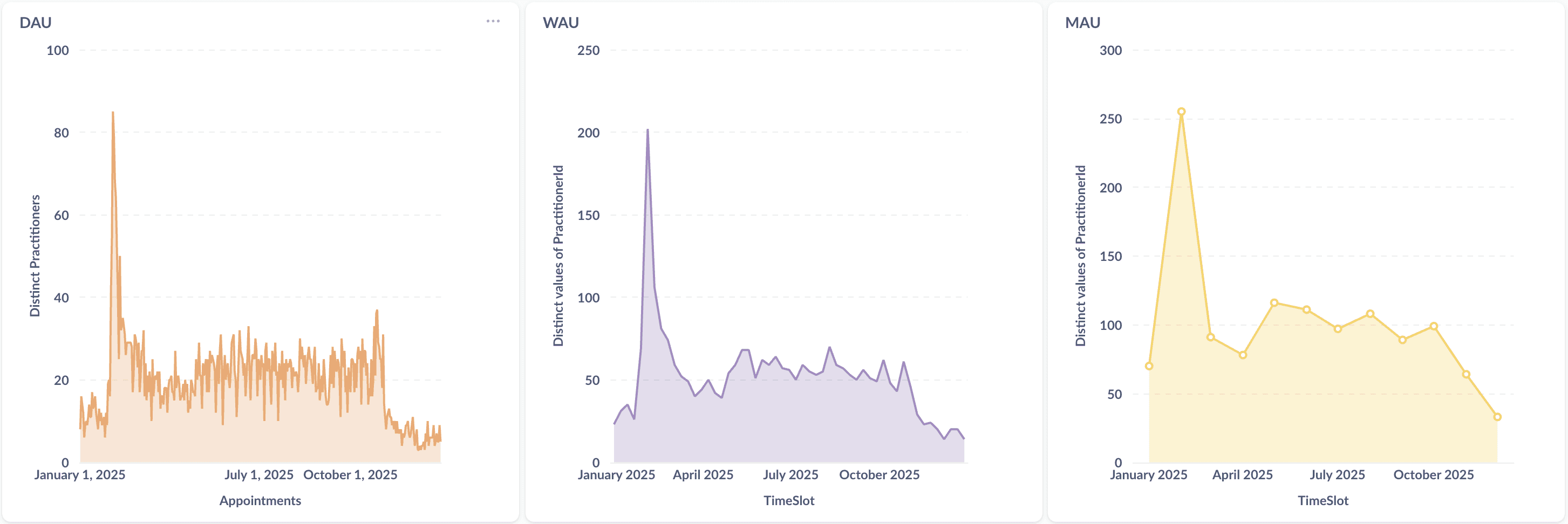
Steady increase in DAU, WAU, MAU between 2023 - 2025
Learnings.
Healthcare requires multiple fluid workflows.
We initially considered outsourcing the engineering since I hadn't coded in over six years. However, as a founder I think it's important to know your product inside out, including how the codebase works.
Human in the lOOP WORKFLOWS are hard to automate.
Workflows that involve patient communication requires humans to confirm that the information being communicated to the patient is accurate. A high degree of unpredictability in patient conditions and possible outcomes makes automation difficult.
Acknowledgements.
ASIRA would not be possible without the combined effort of the engineering, sales and marketing teams. As a small team of three, everyone put in their best work to build India's first eye care specific EMR. A huge thanks to Shirish Kamath for building the initial engineering infrastructure that helps Asira grow and scale with minimal effort.
A big thanks also goes out to Chirag Vyas who interned with ASIRA during the summer of 2023 and who's code is still an integral part of the product.
VISIT ASIRA CLINICAL
Frankensteined in Mumbai.
Fueled by YouTube, 90s cartoons & Heavy Metal.